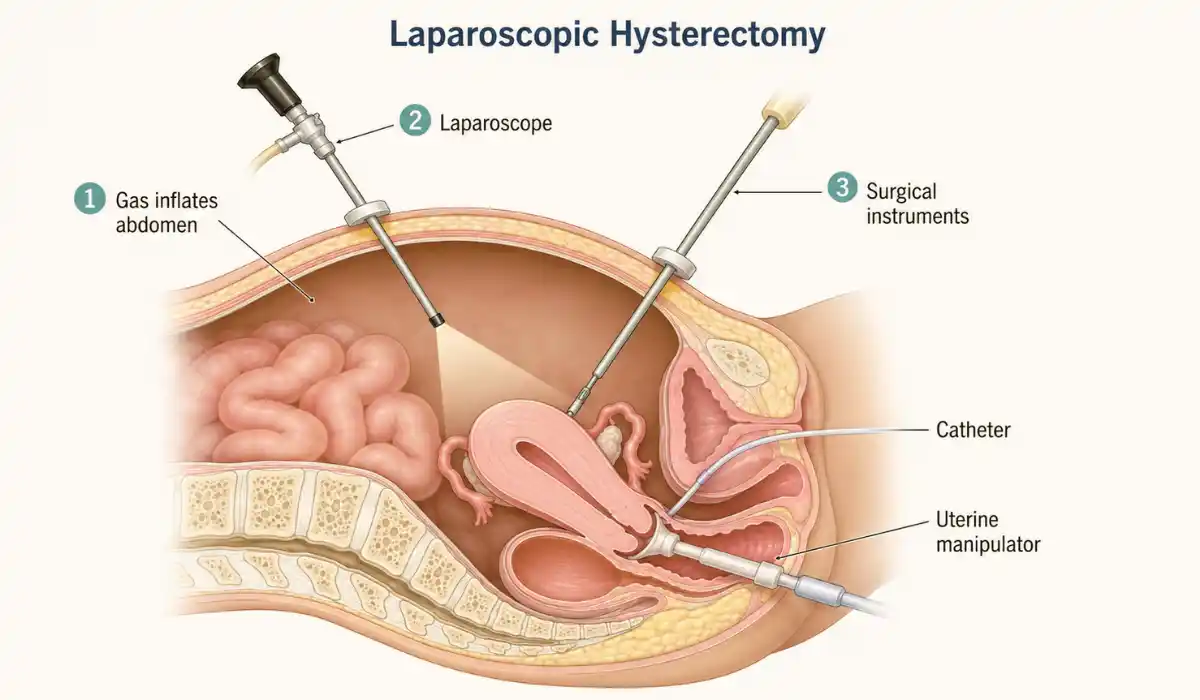
A laparoscopic hysterectomy is an operation that removes the uterus through several small abdominal incisions. A surgeon uses a thin camera called a laparoscope to see inside the pelvis and guide specialized surgical instruments.
This minimally invasive approach usually avoids the large incision used during open abdominal surgery. It can lead to a shorter hospital stay and faster recovery, although it remains a major operation that requires careful planning and follow-up.
What Is a Laparoscopic Hysterectomy?
During the procedure, the surgeon places a laparoscope and surgical tools through small cuts in the abdomen. The uterus is separated from surrounding structures and removed through the vagina or small abdominal openings.
The exact operation depends on the condition being treated. A total hysterectomy removes the uterus and cervix. A supracervical or partial hysterectomy removes the upper uterus but leaves the cervix in place.
The fallopian tubes and ovaries are separate organs. They may be preserved or removed depending on age, medical history, cancer risk, ovarian health, and the reason for surgery.
Is Robotic Surgery the Same?
A robotic hysterectomy is also a type of minimally invasive surgery. The surgeon controls robotic instruments from a nearby console rather than moving the instruments directly by hand.
Both techniques use small abdominal incisions. The best approach depends on the surgeon’s experience, available equipment, uterine size, previous operations, and the condition being treated.
Why Is the Procedure Performed?
A hysterectomy may be recommended for uterine fibroids, adenomyosis, uterine prolapse, severe endometriosis, persistent pelvic pain, or heavy bleeding that has not improved with other treatments.
It may also form part of treatment for cervical, uterine, or ovarian cancer. The surgical method and amount of tissue removed can differ when cancer is present.
A hysterectomy is not always the first treatment considered for a noncancerous condition. Medicines, hormonal birth control, an intrauterine device, uterine artery embolization, endometrial ablation, or other procedures may be appropriate in some cases.
What Happens on the Day of Surgery?
Laparoscopic hysterectomy is usually performed under general anesthesia. The surgeon commonly makes three to five small abdominal incisions and gently expands the abdomen with gas to improve visibility.
The uterus is then detached and removed. The surgeon closes the incisions and, when the cervix is removed, closes the upper vaginal opening with dissolvable stitches.
A urinary catheter may remain in place temporarily. Some patients return home on the same day, while others stay overnight depending on the procedure, medical needs, and early recovery.
Benefits and Possible Risks
Laparoscopic surgery does not require a large abdominal incision. Compared with open surgery, it is generally associated with shorter hospitalization, less postoperative discomfort, and a quicker return to normal activities.
However, every operation carries risks. Possible complications include bleeding, infection, blood clots, reactions to anesthesia, and damage to nearby structures such as the bladder, bowel, ureters, nerves, or blood vessels.
The operation may occasionally need to be changed to open abdominal surgery when unexpected bleeding, scar tissue, organ damage, or limited visibility makes laparoscopy unsafe.
Hormones and Menopause After Surgery
A hysterectomy does not always remove the ovaries. When healthy ovaries remain, they usually continue producing hormones, so immediate menopause does not automatically begin.
When both ovaries are removed, estrogen production drops quickly and surgical menopause occurs. Symptoms can include hot flashes, disturbed sleep, sweating, and vaginal dryness. Treatment decisions should be discussed with the surgical team.
Pregnancy is no longer possible after the uterus is removed. Menstrual periods also stop, although someone who keeps the cervix can occasionally experience light monthly spotting from remaining cervical tissue.
Laparoscopic Hysterectomy Recovery
Laparoscopic hysterectomy recovery commonly takes around two to four weeks after a laparoscopic or robot-assisted total hysterectomy. However, energy levels, internal healing, and activity restrictions can take longer. Recovery time varies based on age, overall health, surgical complexity, and whether additional organs were removed.
Abdominal soreness, tiredness, bloating, light vaginal spotting, and temporary shoulder discomfort from surgical gas can occur. Symptoms should gradually become easier rather than steadily worsening.
Gentle walking is usually encouraged because movement supports circulation and reduces the risk of blood clots. Heavy lifting, strenuous exercise, driving, swimming, tampon use, and sexual activity should wait until the surgeon gives approval.
Practical Preparation and Recovery Tips
Tell your surgical team about all prescription medicines, over-the-counter products, vitamins, and herbal supplements. Follow instructions about fasting and which medicines to take on the day of surgery.
Arrange transportation and help with meals, childcare, shopping, and household tasks. Keep frequently used items within easy reach so you do not need to stretch or lift during early recovery.
A Partial Hysterectomy Guide can help readers understand how this procedure differs from a total hysterectomy. It explains what is removed, whether the ovaries remain, possible hormone changes, recovery expectations, and the warning signs that require medical attention.
When to Seek Professional Help?
Contact your surgeon if pain becomes worse, prescribed medicine does not help, or the incision becomes warm, red, swollen, or begins draining. Fever, repeated vomiting, painful urination, difficulty urinating, foul-smelling discharge, or bleeding heavier than light spotting also require medical advice.
Seek urgent care for difficulty breathing, chest pain, fainting, sudden heavy bleeding, or pain and swelling in one leg. These symptoms can indicate a serious complication such as major bleeding or a blood clot.
Final Thoughts
A laparoscopic hysterectomy removes the uterus through small incisions and usually offers a shorter recovery than open abdominal surgery. The cervix, ovaries, and fallopian tubes are not automatically removed in every procedure.
Ask your surgeon exactly what the operation will involve, why it is recommended, and which alternatives remain available. Clear instructions about recovery, activity, hormone changes, and warning signs can make the healing period easier to manage.
FAQs
A laparoscopic hysterectomy removes the uterus through small abdominal incisions using a camera and specialized instruments. The cervix, tubes, or ovaries may also be removed.
Many people return to light activities within days, but full recovery commonly takes two to four weeks. Your surgeon may restrict lifting and vaginal activity longer.
You will not have uterine periods after hysterectomy. Light spotting can occur during healing, and occasional monthly spotting may continue afterward if the cervix remains.
Menopause does not begin immediately when healthy ovaries remain. Removing both ovaries causes surgical menopause because estrogen and progesterone levels fall quickly after the operation.
Pain is usually manageable and often improves each day. Abdominal soreness, bloating, fatigue, temporary shoulder discomfort from surgical gas, and light vaginal bleeding can occur afterward.
Contact your surgeon for fever, worsening pain, heavy bleeding, foul discharge, wound redness, urinary difficulty, vomiting, breathing problems, or swelling and pain in one leg.




