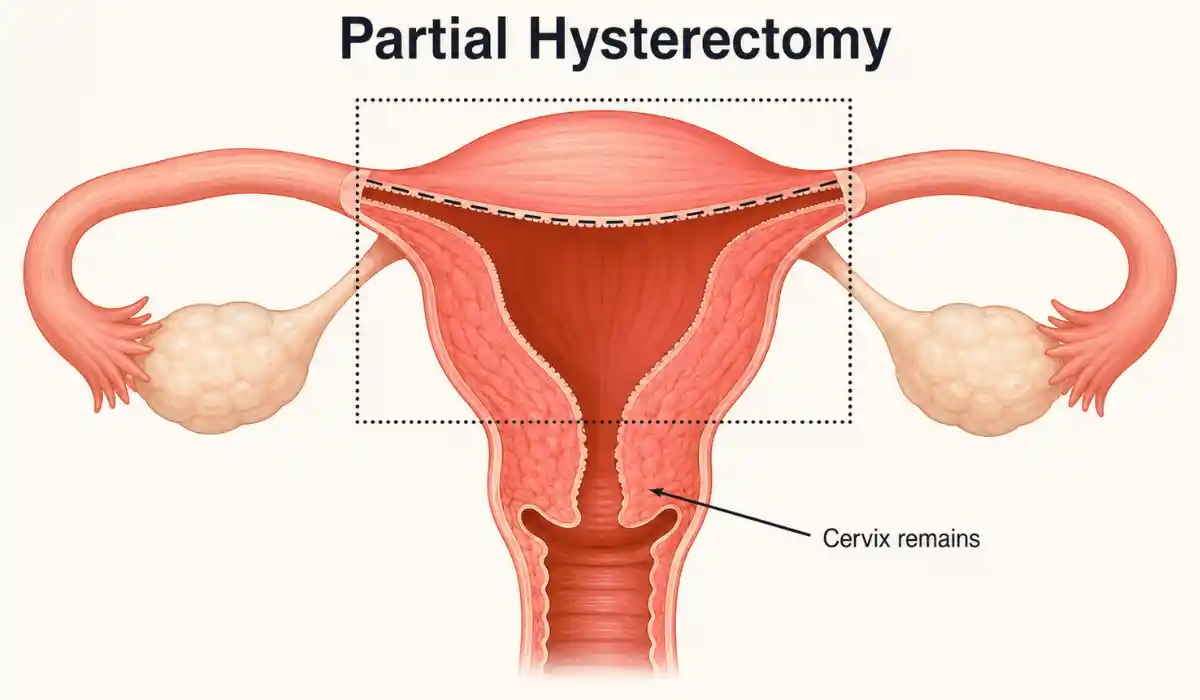
A partial hysterectomy is surgery that removes the upper part of the uterus while leaving the cervix in place. It is also called a supracervical or subtotal hysterectomy. The ovaries and fallopian tubes are separate organs, so they may be kept or removed depending on the reason for surgery.
The procedure permanently ends the ability to carry a pregnancy. Most menstrual bleeding stops, although some people continue to notice light monthly spotting from tissue near the cervix. Understanding exactly which organs will be removed is an important part of planning surgery.
What Does a Partial Hysterectomy Remove?
The surgeon removes the main body of the uterus but preserves the cervix, which is the lower part that opens into the vagina. A total hysterectomy removes the uterus and cervix, while a radical hysterectomy removes additional surrounding tissue.
The terms partial and total do not describe what happens to the ovaries. One or both ovaries may remain, and the removal of the fallopian tubes is also a separate decision.
Will Hormone Levels Change?
When healthy ovaries remain, they usually continue producing hormones until natural menopause. A partial hysterectomy therefore does not automatically cause immediate menopause, although ovarian function can sometimes decline earlier after surgery.
If both ovaries are removed, estrogen levels fall quickly and surgical menopause usually begins. Possible symptoms include hot flashes, sleep changes, vaginal dryness, and mood changes. Discuss the benefits and risks of ovary removal before the procedure.
Why Might the Procedure Be Recommended?
A hysterectomy may be considered for large fibroids, persistent abnormal bleeding, endometriosis, adenomyosis, pelvic pain, or uterine prolapse when other treatments have failed or are unsuitable. Whether the cervix can remain depends on the diagnosis, previous cervical tests, and surgical plan.
A partial procedure is not appropriate for everyone. When cancer or precancer may involve the uterus or cervix, the surgeon may recommend removing the cervix and additional tissue. A supracervical procedure is not recommended for certain precancerous endometrial conditions.
How Is the Surgery Performed?
The operation may be completed through an abdominal incision or with laparoscopic or robot-assisted techniques using smaller incisions. The safest route depends on uterine size, scar tissue, previous operations, the condition being treated, and the surgeon’s experience.
Minimally invasive surgery often allows faster recovery than open abdominal surgery, but it is not suitable in every case. Ask why a particular route is being recommended and what recovery is likely to involve.
Benefits and Possible Risks
The expected benefit is relief from the condition that made surgery necessary, such as heavy bleeding, fibroid pressure, or persistent pelvic discomfort. The likely outcome depends on the original diagnosis and whether other conditions are contributing to the symptoms.
Possible surgical risks include bleeding, infection, blood clots, reactions to anesthesia, and injury to the bladder, bowel, or ureters. Keeping the cervix may also leave a chance of monthly spotting or future cervical health problems.
Because the cervix remains, routine cervical cancer screening is usually still needed. The schedule depends on age, medical history, and previous HPV or Pap test results.
Recovery After Surgery
Recovery depends on the surgical method and your overall health. Mild abdominal soreness, fatigue, bloating, and temporary back pain after hysterectomy can occur as the body heals and activity levels change.
Light spotting, mild abdominal discomfort, bloating, and temporary bowel changes can occur during early recovery. Follow the surgeon’s instructions about driving, lifting, exercise, sex, bathing, and inserting anything into the vagina.
Practical Safety and Recovery Tips
Take prescribed medicines as directed and care for the incision according to the discharge instructions. Gentle walking supports circulation, but strenuous exercise and heavy lifting should wait until the surgical team gives approval.
Drink enough fluids and eat fiber-rich foods to reduce constipation. Keep follow-up appointments and confirm which organs were removed, when cervical screening is due, and when normal activities can safely restart.
Before surgery, ask whether medicine, myomectomy, endometrial ablation, uterine artery embolization, or pelvic floor treatment could address the underlying problem.
Laparoscopic hysterectomy recovery is often shorter than recovery after open abdominal surgery, although tiredness and soreness can still continue for several weeks.
When to Seek Professional Help?
Contact the surgical team if pain worsens, medicine does not help, or the incision becomes red, hot, swollen, or starts draining. Fever, foul-smelling discharge, bleeding heavier than light spotting, painful urination, repeated vomiting, or difficulty passing stool or gas also need medical advice.
Seek urgent care for difficulty breathing, chest pain, fainting, sudden heavy bleeding, or swelling and pain in one leg. These symptoms can indicate a serious postoperative complication.
Final Thoughts
A partial hysterectomy removes the upper uterus while preserving the cervix. It prevents future pregnancy, but it does not always remove the ovaries or cause immediate menopause.
The decision should reflect the diagnosis, treatment goals, cervical health, and risks of each option. Knowing what will be removed and what follow-up is required can make recovery easier to manage.
FAQs
Most people stop having regular periods because the main uterus is removed. However, light monthly spotting can continue when a small amount of cervical tissue remains.
A partial hysterectomy does not automatically remove the ovaries. If they remain healthy, they usually continue producing hormones and immediate surgical menopause is less likely.
No. Removing the uterus means pregnancy can no longer occur, even when the cervix, ovaries, or fallopian tubes remain in the body after the operation.
Yes. Because the cervix remains, routine cervical cancer screening is usually still needed. Your clinician will recommend timing based on age and previous test results.
Recovery varies by surgical route and personal health. Many laparoscopic patients recover within several weeks, while an open abdominal procedure often requires four to six weeks.
Contact your surgeon for heavy bleeding, fever, worsening pain, foul-smelling discharge, breathing difficulty, painful urination, leg swelling, or redness and drainage around the surgical incision.




